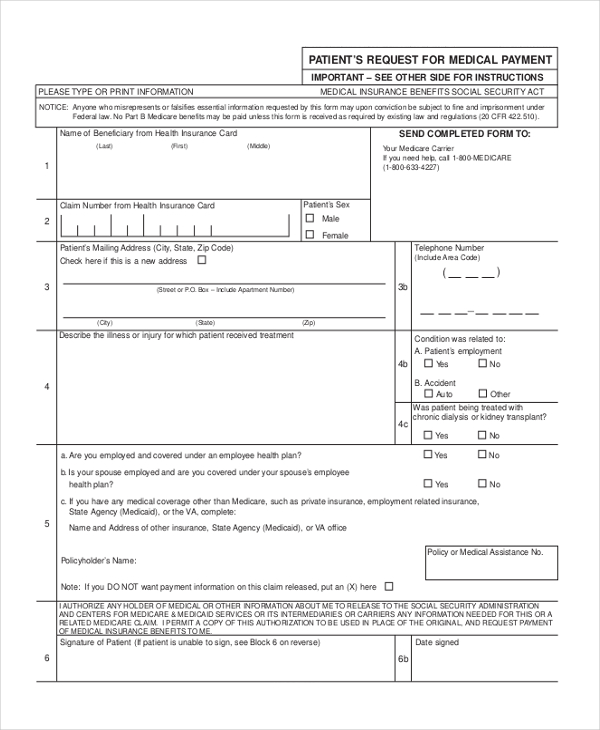
Fill out the Patient Request for Medical Payment form CMS-1490S. You must carefully read and fill out each part of the form or else Medicare will send it.
 Free 6 Sample Medicare Reimbursement Forms In Pdf
Free 6 Sample Medicare Reimbursement Forms In Pdf
The Medicare reimbursement form also known as the Patients Request for Medical Payment is available in both English and Spanish on the Medicare website.

Medicare reimbursement form. Reimbursement form Your itemized receipts Please submit these items to. Complete a separate form. To receive a reimbursement you must.
I am requesting reimbursement for Medicare Part B premium expenses incurred by myself or my dependents while I was a member of the MVP Health Care Standard Option plan. How to Get Reimbursed From Medicare. You can download the reimbursement form at Medicares website or at the link below.
We pay Medicare benefits directly into your nominated bank account. Youll find the address for form submission in the instructions. Find your best rate from over 4700 Medicare plans nationwide.
The form is called the Patient Request for Medical Payment form. MEDICARE REIMBURSEMENT ACCOUNT MRA CLAIM FORM INSTRUCTIONS HOW TO SUBMIT CLAIMS BY FAX OR MAIL IMPORTANT Dont include this instruction page with your faxed or mailed claim form. MEDICARE REIMBURSEMENT ACCOUNT MRA CLAIM FORM INSTRUCTIONS HOW TO SUBMIT CLAIMS BY FAX OR MAIL Proof of premium payment such as a cleared check bank statement or credit card IMPORTANT.
This can be for a paid or unpaid account. When a provider accepts assignment they agree to accept. Medicare Claim form MS014 Use this form to claim Medicare benefits by mail or in person at a service centre.
Find your best rate from over 4700 Medicare plans nationwide. Fill out this form if youre asking for a medical dental eyewear hearing aid or vaccine reimbursement and you paid a doctor healthcare professional or service provider who did not bill us directly. FILLING OUT YOUR CLAIM FORM.
Dont use this form for prescription drug claim reimbursements. Submit one Medicare Part B Reimbursement Request Form to set up recurring reimbursement for the rest of the year. Once you receive the EOB complete this form submit the pharmacy receipts and attach the EOB.
Annons Find affordable quality Medicare insurance plans that meet your needs. If you still do not know the address of your Medicare contractor call 1-800-MEDICARE 1-800-633-4227. Medica Claims PO Box 30990 Salt Lake City UT 84130 Questions.
Reference the Medicare Administrative Contractor Address table for the correct address to mail your claim form. Send the completed form and supporting documentation to your Medicare contractor. How to complete this Medical Claim Reimbursement Form When to use this form.
This form is available both in English and Spanish. Application for a Medicare Entitlement Statement form MS015 Application to copy or transfer from one Medicare card to another form MS011 Application to receive the Australian Government Rebate on Private Health Insurance as a reduced premium form MS006. The EOB must clearly indicate the cost of the prescription and amount paid by the primary plan or Medicare.
U Complete this claim form u Attach your itemized receipts u Submit within 365 days from the date of purchase u Allow 4 to 6 weeks for processing u Send the completed form and a copy of your receipts to. FILLING OUT YOUR CLAIM FORM 1. I have notwill not seek reimbursement of this expense from any other plan or party.
Your plan covers dental services from licensed dentists within your service area up to an annual limit. I want to file a claim for services andor supplies that I got Patient Request for Medical Payment formCMS-1490S. Guide to Recurring Medicare Part B Reimbursement Requests This form is for those who want to be automatically reimbursed monthly for their premiums deducted from their Social Security benefit check.
To get reimbursement you must send in a completed claim form and an itemized bill that supports your claim. Below you will find a variety of Medicare forms including a Medicare appeal form Medicare opt-out. Medicare forms allow you to sign up for Medicare to end your Medicare coverage to dispute a payment decision to consent to a home a visit and more.
The Centers for Medicare and Medicaid CMS sets reimbursement rates for all services and equipment provided to Medicare recipients. Download and complete the Medicare Claim form. TTY users should call 1-877-486-2048.
Please include your bank details on the form if we dont have them or if they need. To receive reimbursement please submit the following. Submit the claim to the primary plan or Medicare.
I certify that the information on this form is accurate and complete. Refer to your Evidence of Coverage for your plans limit. Dont include this instruction page with your faxed or mailed claim form.
Annons Find affordable quality Medicare insurance plans that meet your needs. Account Holder Information Please print or write legibly when completing the account holder first and last name.



