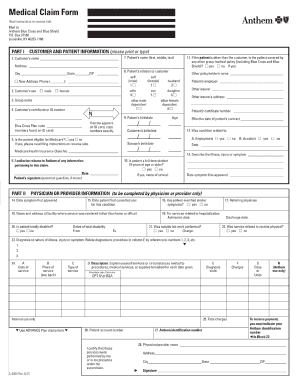
Complete all areas of the Claim Form before returning the claim to us. If you are a member of a group practice the services of all physicians in your group can be reported on one claim form if the first 11 digits of the Anthem identification numbers are the same.
 Anthem Medical Claim Form Fill Online Printable Fillable Blank Pdffiller
Anthem Medical Claim Form Fill Online Printable Fillable Blank Pdffiller
Please complete the form.
Anthem medical claim form. Call our State of Connecticut Enhanced Member Service Unit at 1-800-922-2232. State of Connecticut Dedicated Service Unit Anthem Blue Cross Blue Shield PO. Your cooperation in completing all items on the claim form and attaching all required documentation will help expedite quick and accurate processing.
2 of 2 HOW TO USE THIS FORM Dear Member. Please send claims to. Use a separate claim form for each patient and each physicianprovider rendering services.
Recheck all information and submit this form along with supporting material to. Browse commonly requested forms to find and download the one you need for various topics including pharmacy enrollment claims and more. If for some reason your health care professional cannot file the claim on your behalf you may use this form to claim benefits.
You can use Availity to submit and check the status of all your claims and much more. Monday through Friday from 800 am. Please send claims to.
SEE REVERSE SIDE FOR COMPLETE INSTRUCTIONS. Keep a duplicate copy of your itemized bills as they will not be returned to you. See reverse side for complete instructions.
533935 29271VAMENABS Anthem HK Member Claim Prt FR 05 12 This claim form is designed to help you the member or your health care professional file your itemized health care related bills. 312017 94928 AM. Be sure the following information is provided.
Box 17849 Denver Colorado 80217-0849. Log in to Availity. Box 105187 Atlanta GA 30348-5187 If you have questions or need any assistance please call the number listed on your Member ID card.
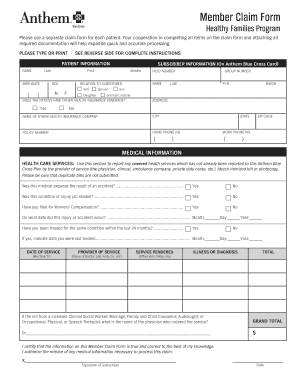
The information on this Medical Claim Form is true and correct. I authorize the release of any medical information necessary to process this claim. Member Claim Form Please use a separate claim form for each patient.
Medical records are requested when additional information is needed in order to process a claim. Letters sent to. Filing your claims should be simple.
Comply with our simple actions to have your Anthem Medical Claim Form ready quickly. Of knowing about your claim. Anthem Health Plans Inc.
Overseas members should use the Overseas Medical Claim Form. An independent licensee of the Blue Cross and Blue Shield Association. Anthem Blue Cross and Blue Shield is the trade name of Anthem Health Plans of Virginia Inc.
Your cooperation in completing all items on the claim form and attaching all required documentation will help expedite quick and accurate processing. Anthem Blue Cross and Blue Shield PO Box 54139 Los Angeles CA 90054-0139 Anthem Blue Cross and Blue Shield is the trade name of. Medical Claim Form instructions.
We are happy to serve you. Patient information Use this section to identify the patient. Signature Name Date MMDDYYYY X.
Anthem Blue Cross and Blue Shield PO. PATIENT INFORMATION Last name First name. International Claim Form Health Insurance Blue Cross Blue Shield Global Core Blue Cross Blue Shield Global Core Created Date.
Include itemized bills prepared by those who have rendered the services. Find the web sample from the library. Type all required information in the necessary fillable fields.
Not bill us directly complete the claim form attach itemized bills and mail the white copy to Anthem Blue Cross and Blue Shield PO. Rocky Mountain Hospital and Medical Service Inc. Your cooperation in completing all items on the claim form and attaching all required documentation will help expedite quick and accurate processing.
If you use a provider outside of the network you will need to complete and file a claim form for reimbursement. Select ProviderStateAnswersAnthemProvider Adjustment Form. HMO products underwritten by HMO Colorado Inc.
Thats why Anthem uses Availity a secure full-service web portal that offers a claims clearinghouse and real-time transactions at no charge to healthcare professionals. 3352701 24066MUMENABS ABS Medical Claim Prt FR 01 19 R2 Please use a separate claim form for each patient and provider. Sign and date claim form.
Registered marks Blue Cross and Blue Shield Association. The easy-to-use dragdrop user interface makes it easy to add or move fields. Health Benefits Claim Form.
This Medical Claim Form was developed to notify us of any covered health service for which we have not already been billed. The form is available in both an Adobe Acrobat and MSWord versions for your convenience. If benefits are to be claimed for more than one family member a separate claim form must be submitted for each member.
673233 24066CEMENABS ANA Central Medical Claim Prt FR 10 12 Please use a separate claim form for each patient and provider. Most health care professionals will file claims for you. ANA EAST-WEST MEDICAL CLAIM FORM INSTRUCTIONS.
Anthem Blue Cross is the trade name of Blue Cross of California. Please read the following instructions about how to report Health Care Services. Medical Records Associated with Local Claims.
Independent licensee of the Blue Cross Association. SEE REVERSE SIDE FOR COMPLETE INSTRUCTIONS.


/UB04-57a5d9773df78cf459cd0ef3.jpg)