However some plans require an additional monthly premium for drug coverage. The Request for Reconsideration of Medicare Prescription Drug Denial model notice has been updated to include C2Cs contact information as they are the Part D QIC effective 020121.
 Free Medicare Prior Rx Authorization Form Pdf Eforms
Free Medicare Prior Rx Authorization Form Pdf Eforms
If you wish to request a Medicare Part Determination Prior Authorization or Exception request please see your plans website for the appropriate form and instructions on how to submit your request.
Medicare part d prior authorization form. Medicare Part D Medications Express Scripts manages prior authorizations and Non-Formulary requests for Medicare Part D prescriptions. Submit online at Express Scripts or call 1-800-935-6103. Patient home telephone number.
OptumRx Prior Authorization Department PO. I further attest that the information provided is accurate and true and that documentation supporting this. Express Scripts Medicare PDP Enrollment PO.
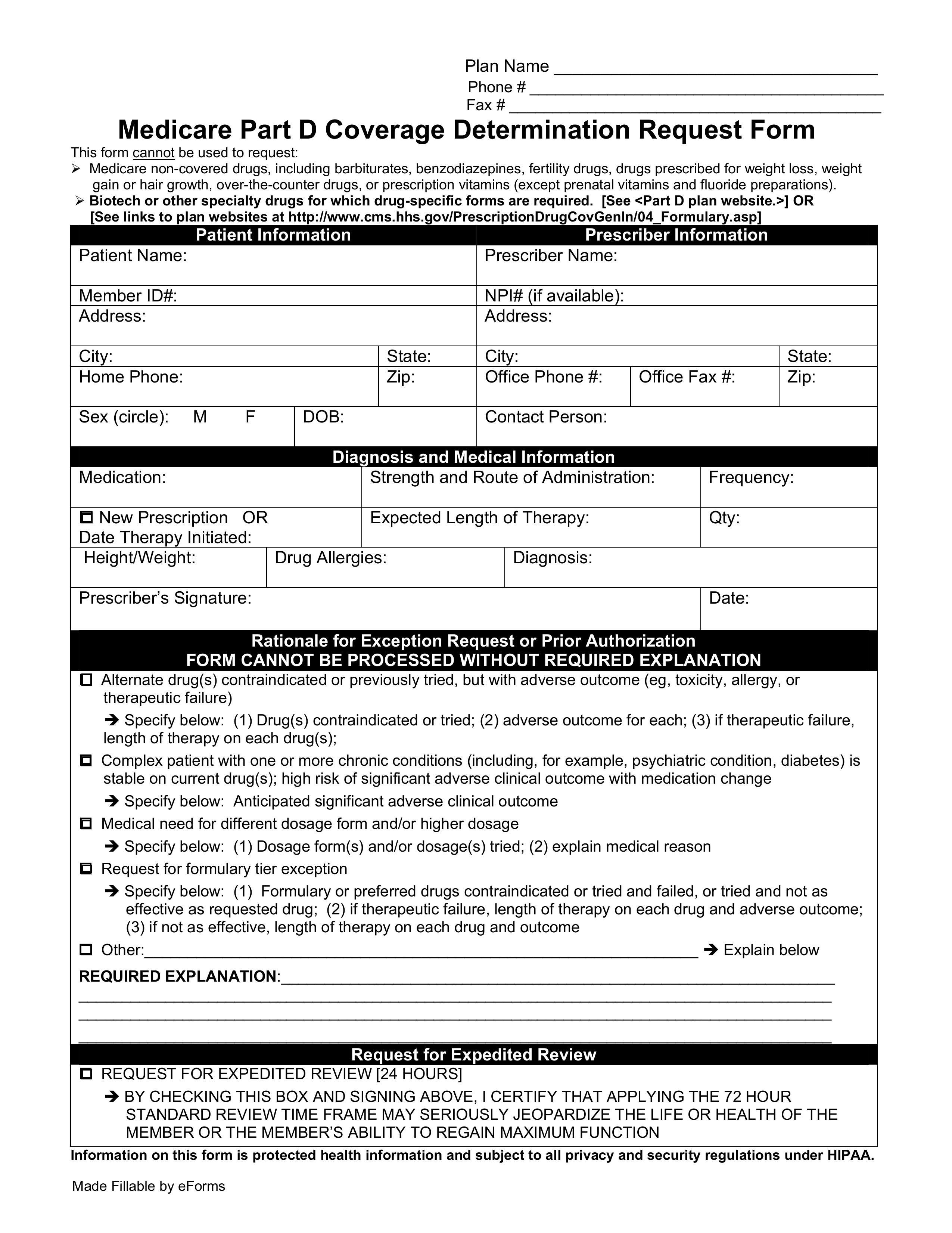
Exception to Prior Authorization Request. REQUEST FOR MEDICARE PRESCRIPTION DRUG COVERAGE DETERMINATION. Medicare Part D Coverage Determination Request Form.
This form can be used to request reimbursement for a covered prescription or vaccine that you purchased without using your Medicare Part D member ID card. Whose prescription drug coverage was sold in the state of Colorado. For urgent requests please call.
PLEASE FAX COMPLETED FORM TO 1-888-836-0730. You may also use this form to join Express Scripts Medicare. Santa Ana CA 92799.
It also includes a Pre-Enrollment Checklist of important things to consider before you enroll. Who reside in the state of Colorado andor. Enrollment forms I have Part A and want to apply for Part B Application for Enrollment in Part BCMS-40B.
The use of this form is mandated for prior authorization requests concerning commercial fully insured members. Print our online Medicare Part D enrollment form and then complete and mail it to. I attest that the medication requested is medically necessary for this patient.
Once a patient or their physician receives a written denial coverage determination they should submit a coverage determination request form asking for the drug. The Medicare Prior Rx Authorization Form or Drug Determination Request Form is used in situations where a patients prescription is denied at the pharmacy. Outpatient Authorization Request Form.
Recommended that CMS implement a standard Prior Authorization PA form to facilitate coordination between Part D sponsors hospices and prescribers. Information on this form is protected health information and subject to all privacy and security regulations under HIPAA. A WellCare Prior authorization form is a document used for requesting certain prescription drugs or coverednon-covered services.
In March 2014 CMS guidance included a list of data elements that would be expected to be used in a Part D hospice PA form or documented by the sponsor when received verbally. You may also ask us for a coverage determination by calling the member services number on the back of your ID card. Uniform pharmacy prior authorization request form PDF opens new window.
Get the SF-5510 as a PDF form in Spanish or HMTL form in Spanish. Patient address city state ZIP. 2020 Request for Medicare Prescription Drug Coverage Determination Page 1 of 2 You must complete both pages Fax completed form to.
5302017 122819 PM. Medicare Part D Coverage Determination Request Form PDF 38751 KB For certain requests youll also need a supporting statement from your doctor. Fill out the Application for Enrollment in Part B CMS-40B.
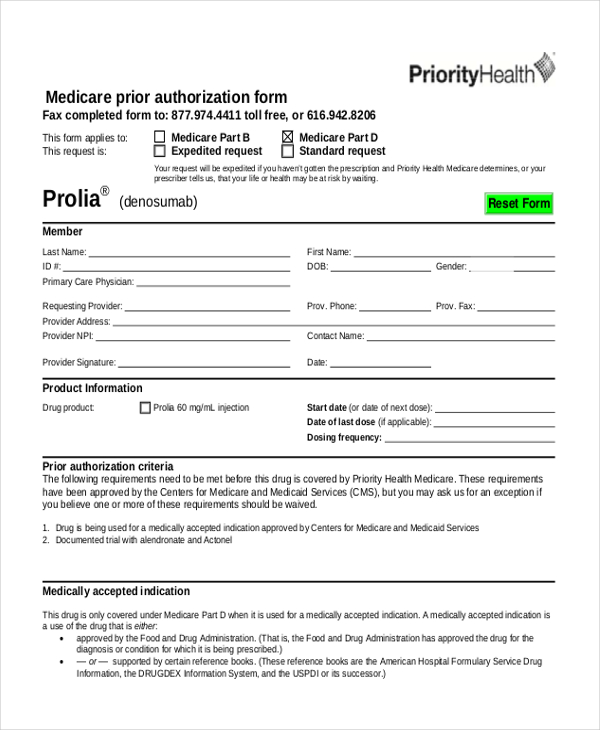
Authorized Representative Request PDF Medicare Member Authorization Appeal-appealing Medicare denials of medical prior authorization precertification requests PDF Medicare Non-contracted Provider Appeal Process PDF Medicare Appeals Provider Memo- Post Service PDF. Request for Medicare Prescription Drug Coverage Determination - Medicare Fill out and submit this form to request prior authorization PA for your Medicare. View Part D prior authorization requirements.
Box 4345 Scranton PA 18505. There are also forms for filing an appeal or letting Medicare share your personal health information. This form may be sent to us by mail or fax.
Contact CVS Caremark Prior Authorization Department Medicare Part D. 1-844-403-1028 Prior Authorization Department. Get Medicare forms for different situations like filing a claim or appointing a representative.
View print or order Medicare publications and listen to podcasts. You may download this form by clicking on the link in the Downloads section below. Members of Medicare Advantage MA Plans typically receive Part D coverage automatically.
Box 25183 Santa Ana CA 92799. For Part D prior authorization forms please see the Medicare section. Fill out the Authorization Agreement for Pre-authorized Payments form SF-5510 as a PDF in English or HTML in English.
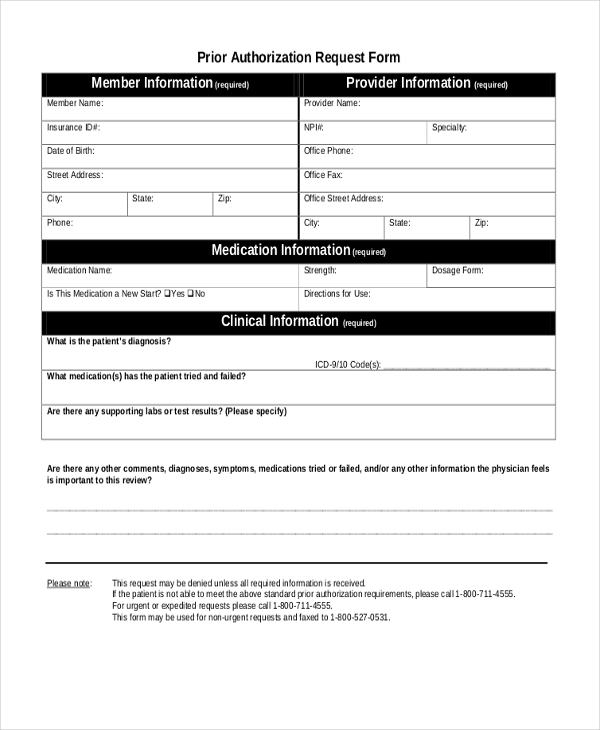
Requests for prior authorization with supporting clinical information and documentation should be sent to ʻOhana 14 days prior to the date the requested services will be performed. Patient information Patient name Patient insurance ID number.
 Medco Medicare Part D Prior Authorization Form Best Of Top Result 59 Unique Medco Express Scripts Prior Authorization Form Models Form Ideas
Medco Medicare Part D Prior Authorization Form Best Of Top Result 59 Unique Medco Express Scripts Prior Authorization Form Models Form Ideas
 Advantra Silver Prior Auth Form Fill Online Printable Fillable Blank Pdffiller
Advantra Silver Prior Auth Form Fill Online Printable Fillable Blank Pdffiller
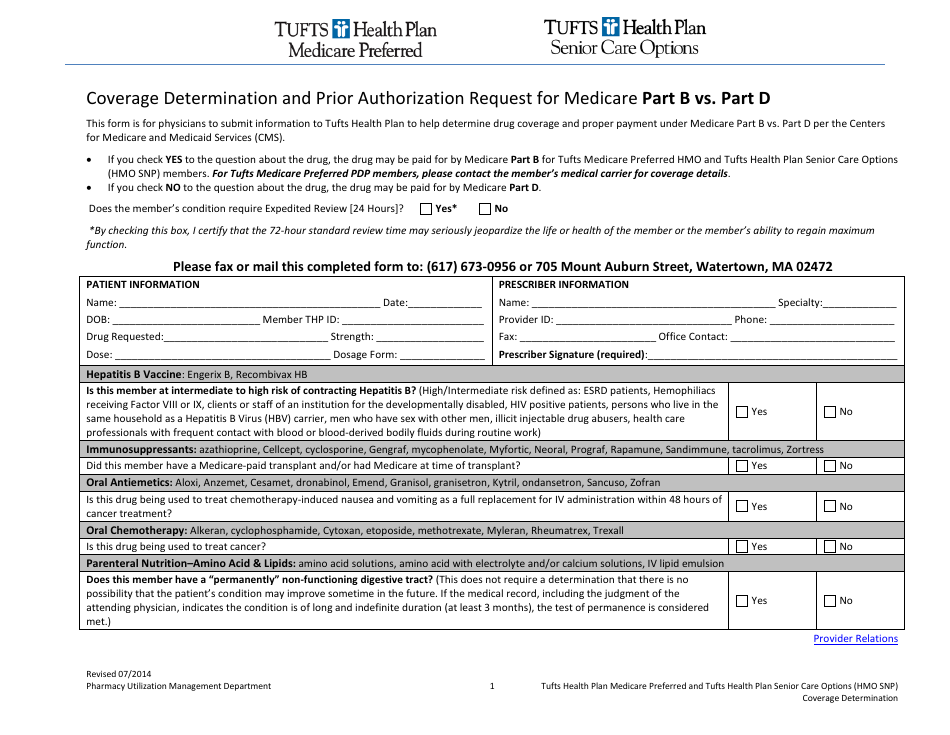 Coverage Determination Form And Prior Authorization Request For Medicare Part B Vs Part D Tufts Download Fillable Pdf Templateroller
Coverage Determination Form And Prior Authorization Request For Medicare Part B Vs Part D Tufts Download Fillable Pdf Templateroller
 Free 10 Sample Medicare Forms In Pdf Ms Word
Free 10 Sample Medicare Forms In Pdf Ms Word
Https Www Express Scripts Com Art Medicare16 Pdf Coveragereviewfaxform Pdf
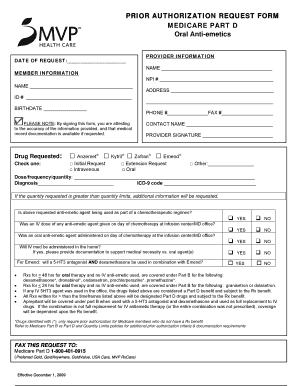 Mvp Prior Auth Form Fill Online Printable Fillable Blank Pdffiller
Mvp Prior Auth Form Fill Online Printable Fillable Blank Pdffiller
 Free 8 Sample Prior Authorization Forms In Pdf Ms Word
Free 8 Sample Prior Authorization Forms In Pdf Ms Word
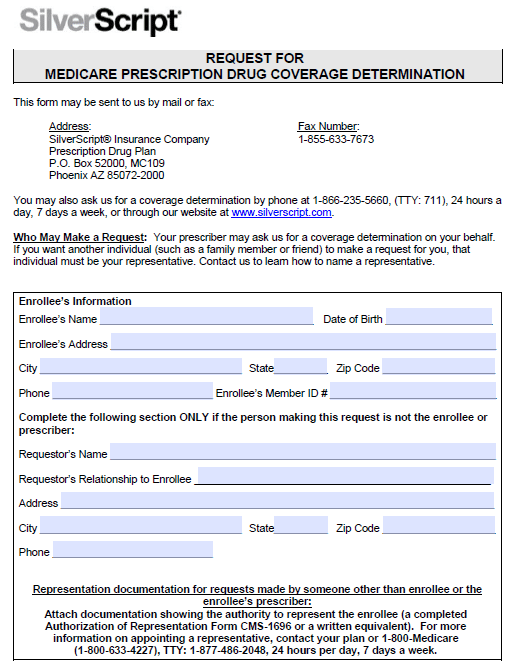 Silverscript Prior Prescription Rx Authorization Form Authorization Forms
Silverscript Prior Prescription Rx Authorization Form Authorization Forms
 Fillable Online Medicare Part D Prior Authorization Form Fax Email Print Pdffiller
Fillable Online Medicare Part D Prior Authorization Form Fax Email Print Pdffiller
Https Www Bcbsal Org Pdfs Egwp S1030 Pda Egw 13 Wb Pdf
 Fillable Online Prior Authorization Form Prior Authorization Form For Medicare Plan Part B And Part D Fax Email Print Pdffiller
Fillable Online Prior Authorization Form Prior Authorization Form For Medicare Plan Part B And Part D Fax Email Print Pdffiller
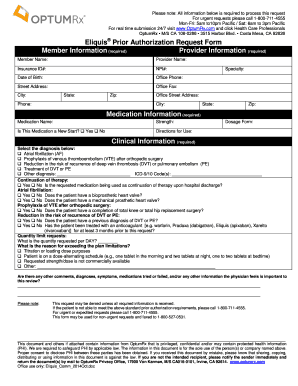 Optumrx Prior Authorization Form Fill Online Printable Fillable Blank Pdffiller
Optumrx Prior Authorization Form Fill Online Printable Fillable Blank Pdffiller
 Medco Prior Authorization Form Fill Out And Sign Printable Pdf Template Signnow
Medco Prior Authorization Form Fill Out And Sign Printable Pdf Template Signnow
Https Www Bcbsal Org Web Documents 1511503 9929544 S1030 Pda Egw 14 Part D Drugauthreq Pdf D085207b 179b 4f5c Be8c 81a625901e12




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.